
What Smoking Really Does During Pregnancy
You might know that smoking is bad during pregnancy. Here’s what you may not know.

Busy Exam Season for Kids? Keep Oral Health on Track
April and May are busy exam months for many students and their families. Stress, late night studying and sugary snacks and energy drinks can affect your child’s oral health. A few simple habits can help protect their smile during a stressful time.

The Basics of Dental Implants
While dental implants can replace missing teeth, patients should talk to their dentist about the pros, cons and costs before deciding.

Understanding and Preventing Tooth Enamel Erosion
Taking care of your tooth enamel is important for keeping your teeth healthy and avoiding problems in the future.

Mouthwash and Your Oral Health Routine
Mouthwash can complement your oral hygiene routine. Learn the key differences between alcohol and alcohol-free options for maintaining optimal oral health.

Taking Care of Your Teeth While Traveling
Practice proper oral care even when away from home.

Why Your Child Needs a Dental Home
Establishing a dental home by your child's first birthday provides essential preventive care, education and long-term oral health benefits that contribute to overall wellness throughout their life.

Exercise and Your Oral Health
Exercise improves both your overall health and oral health. Our practical tips will help you protect your smile while staying active.

Teen Oral Health
Get essential guidance on teen oral health, from proper brushing techniques and orthodontic care to avoiding harmful habits and protecting teeth for the future.

Breast Feeding and Oral Health: What Moms Should Know
Breastfeeding benefits both maternal health and baby's oral development.
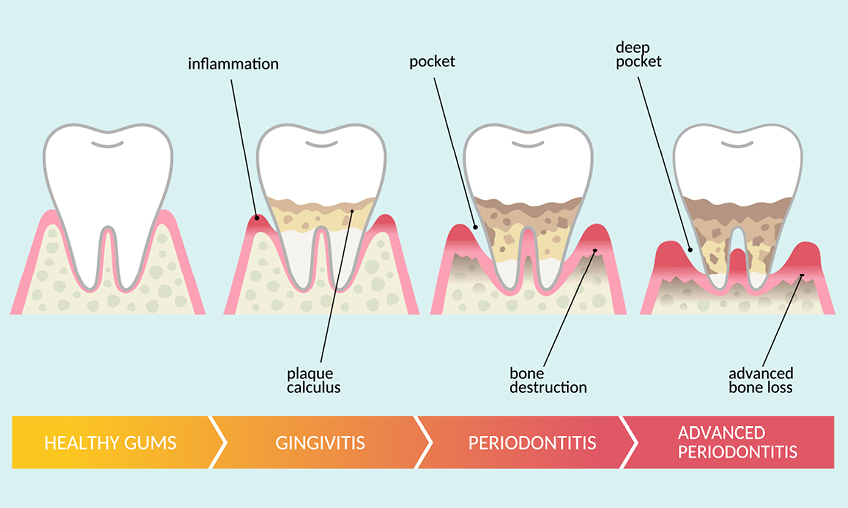
Know How Gum Disease Happens and How You Can Resist It
Periodontal disease can sneak up on you. It’s never too late or too early to know and address the signs to protect your oral health.

Toothache? Get Assistance and Relief for Tooth Pain
Here’s why toothaches happen, how to feel better ASAP, when to visit the dentist and what to do when your pain is unbearable.
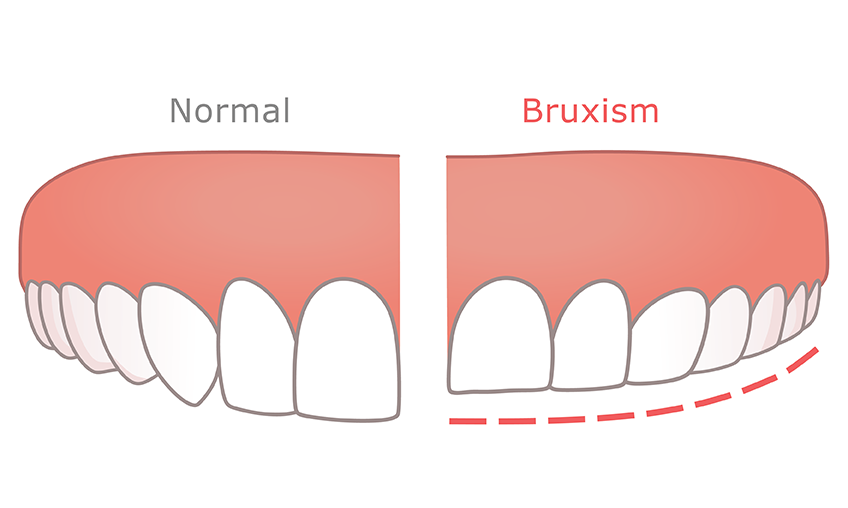
Teeth-Grinding: Get Help for Pain and Discomfort
Know the signs and causes of bruxism, which can hurt your teeth, jaw and more over time.
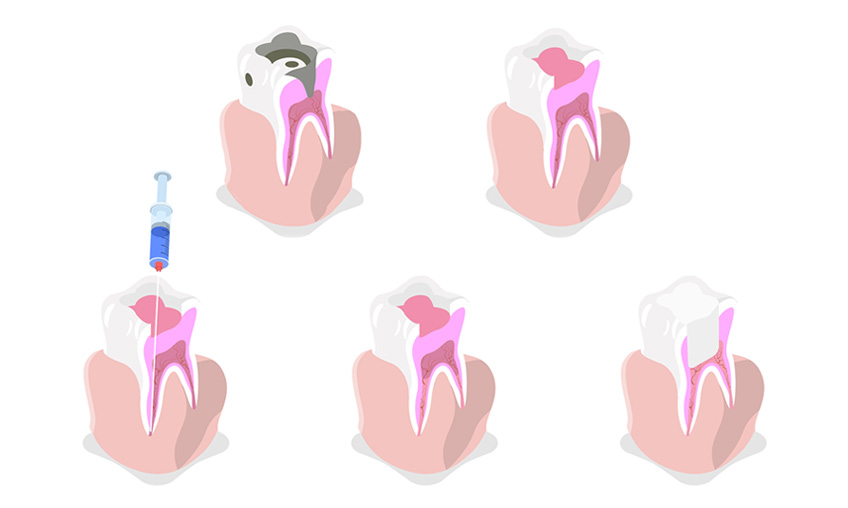
Root Canals and Dental Crowns: What to Know, What to Expect
Here’s why people get root canal therapy and dental crowns, and what the experience is like.

Four Tips To Avoid Jack-O-Lantern Teeth This Halloween
Four tips for making it through Halloween with healthy teeth and good oral hygiene.

What Every Pregnant Woman Should Know About a Healthy Mouth
Congratulations on your pregnancy! Prenatal dental care for you and your baby is important.

Setting Fun Resolutions with Kids
The secret to setting family resolutions that stick? Don’t take them seriously.

Enjoy the Holidays While Protecting Your Oral Health
Enjoy the holiday season with tips and recipes to boost your oral health and overall wellness.
Healthy Teeth and Gums at 60 and Beyond
Know possible oral health concerns for mature adults. Avoid pain and trouble by taking care of them early.

Vaping and Your Oral Health
Vaping harms the whole body, including your teeth and gums. Free programs can help you quit.

Oral Health for Babies
Follow these helpful tips to support your baby's oral health, even before their first tooth.

How to Stop Bad Breath
Bad breath (also known as halitosis) comes from certain foods, lack of oral hygiene, gum disease, dry mouth, tobacco, or medical problems.

How Gum Disease Can Hurt Your Pregnancy
Here's how to keep gum disease from having a bad impact on pregnancy, childbirth and your baby.

Healthy After School Snacks Your Kids Will Love
After a busy day of learning and playing, kids are hungry! But instead of having them dig into a packaged treat that’s loaded with sugar, offer these healthy options that are a snap to prepare. Sure to delight, these snacks provide energy and nutrition and keep them satisfied until dinner.

Three Techy Tools for Toothbrushing Tantrums
Arm your toothbrushing arsenal with techy distractions and rewards. That way, no matter what type of tantrum happens, you’ll be one smile ahead.

Snack Tips
Eating a lot of snacks that have sugar may give your child cavities.

Sealants Make Sense
Brushing and flossing are the best ways to help prevent cavities. But it’s not always easy to clean every surface of teeth. Back teeth – called molars – have deep grooves that can trap food. This can lead to a buildup of bacteria that over time can cause tooth decay.

Easy Ways to Kick Start Your Child's Oral Health Routine
Did you know that oral health – the health of your teeth and gums – has a major impact on your overall health? It’s true! So if you want to help your child stay healthy, start with their smile. By teaching them to take better care of their mouth, you’re also taking better care of their body. Here are some simple tips that can make a big difference.
Five Ways to Actually Make Brushing their Teeth Exciting
When it’s toothbrushing time at your house, it’s easy to feel like the odds are stacked against you. Some kids do everything they can to avoid it. Some kids brush incorrectly. And others just aren’t feelin’ it. The good news is that there are many ways to make brushing painless, effective, and 100% kid-friendly.

Four Simple Ways to De-stress Your Day
Teaching your kids how to brush their teeth properly twice a day, every day can be stressful. Everything else that you’ve got on your plate (wait, what’s for dinner?!) can interfere with peace of mind, too. We want to help you keep things easier. Here are some of the simple things you can do each day to ward off stress at your house.

Oral Care with Dentures
Dentures require a few small changes to dental habits.
Four Ways to Keep Your Smile Healthy
Take care of your teeth and gums for a healthy smile.

Oral Cancer in Mature Adults
Oral cancer takes time to develop, so it mostly happens in people over 55. Learn the risks and how to protect yourself.

New to Teledentistry? Here’s What to Expect
Teledentistry is an easy new way to get care if you can't get to the dentist's office.

Don't Ghost Your Dentist
Stay on top of oral health and overall wellness when you make the most of your dental appointment.

What to Expect When Returning to the Dentist
As dentists reopen their practices during the COVID-19 pandemic, they are being provided with resources, guidelines and safety protocols from both the American Dental Association (ADA) and the Centers from Disease Control (CDC) for how to move forward.

Prevent Cavities in Early Childhood
Guard against pain and infection for your child with a couple of small changes.
Dental Sealants Prevent Tooth Decay
A dental sealant is a thin coating that protects teeth.

How to Care for Your Dentures
Keep your dentures clean and in good shape.

Tobacco Makes Your Mouth Unhealthy
Using tobacco is always bad news, including for your teeth and gums. Get help with quitting.

FAQs About Oral Health During Pregnancy and Infancy
Understand special oral health concerns during pregnancy, dental benefits for pregnant women and babies, and more.

Why Flossing Is Good for You
Use dental floss once a day for healthy teeth and gums.

Get the Most Out of Your Dental Benefits
Dental coverage is an important part of maintaining your overall health. So prioritizing dental coverage should be a no-brainer, right? We think so!
What to Do if You’re Afraid of the Dentist
If you avoid the dentist because of possible pain or discomfort, these tips can help.
What Is Antimicrobial Mouthwash?
Antimicrobial mouthwash kills bacteria to control or reduce bad breath, gingivitis, plaque and tooth decay. It requires a prescription.

How to Check Your Child’s Teeth
A quick peek can alert you to trouble.
Oral Care for Toddlers (18 to 24 Months)
Encourage your child’s life-long oral health.

Fluoride Protects Against Cavities
Flouride is your child's friend for a lifetime of oral health.

What to Know About Caring for Baby Teeth
Comfort and care make you a real-life Tooth Fairy.
Tooth Decay: How to Prevent It
Follow these simple steps to stop damage to tooth enamel, prevent cavities and benefit from a lifetime of good oral health.

Oral Cancer: What You Need to Know
All about signs, screening, detection and prevention of oral cancer.

Do You Drink Bottled Water?
Why pay extra for something that doesn't help?

Diabetes and Oral Health
A dentist can find signs of Type 2 diabetes during a regular check-up. That's important to help protect your teeth, gums and whole body.

A Caregivers' Guide to Oral Health for People with Disabilities
Here's how caregivers can protect oral health.
FAQs: Pregnant Women and Gum Disease
Gum disease is a special concern when you are pregnant.
Dental Visits with Your Child: What to Do
Get ready, get set, go to the dentist!
Tips for ages 12+ years
Good eating habits, early warning signs of tooth decay and going to the dentist at 12 years and older

Tips for Ages 2-6 Years
Good eating habits, early warning signs of tooth decay and going to the dentist.
Tips for Ages 6-12 Years
Good eating habits, early warning signs of tooth decay and going to the dentist between the ages of 6 and 12 years.
Tips for Ages 6-12 Months
Tips for brushing, baby bottle tooth decay and going to the dentist.

The Haven of Health: Finding Your Dental Services Home
At DentaQuest, we recognize the importance of access to quality dental services — especially for children.

Making the Dentist Less Scary for Your Kids
Going to the dentist can be a real fear for children. Even though it’s common for kids to be afraid, there are ways to make them feel better.
What to Expect at the Dentist's Office
You’ve made your child’s dental appointment and are on your way to helping them have a healthier and happier mouth. Here’s what to expect at your child’s dental visit.

Five Teeth-Staining Foods and Four Tricks to Fight Back
There are many common foods and drinks that can break down enamel and stain your teeth. This can also help cause tooth decay and other issues.
Nutrition and Oral Health — Why You Should Assess Your Diet this National Nutrition Month
Our food choices have a direct connection to another important part of our overall well-being — our oral health.

Kids Oral Health 101 – Baby Teeth Matter
Here are five best practices that all parents and caregivers should know in order to care for their children's oral health

Oral Health Tips for Valentine's Day
As Valentine’s Day approaches, the opportunities for a sugar rush are endless — from conversation hearts to chocolate samplers to pink drinks with sugared rims, our countertops are awash in pink and sweets. But while it’s fun to enjoy these alongside your favorite person or romantic comedy, it’s also important to remember these oral health tips.

Everyday Dental Care with Fluoride
Daily oral care always gets a boost when your toothpaste and mouth rinse contain fluoride.
Your Young Child's Dental Health is Important
Good oral health should start before a baby’s first tooth comes in.
